Table of Contents
- Introduction
- The Overlooked Connection Between Folate and Depression
- Biochemical Mechanisms Linking Folate Deficiency to Depression
- The Need for Further Research and Clinical Considerations
- Take-Home Messages
- Summary and Conclusions
- Did You Know About Folate Receptor Autoantibodies (FRAAs) and Brain Development?
- References

Figure 1. The Folate Factor: Revealing the Hidden Impact on Depression. This figure illustrates the critical role of folate in mental health, highlighting its influence on serotonin synthesis and overall mood regulation. Folate deficiency, prevalent in approximately one-third of individuals with depression, can exacerbate depressive symptoms by disrupting serotonin production and lowering levels of S-adenosylmethionine (SAMe), a compound with known antidepressant properties. The signs and symptoms of depression, such as decreased appetite, weight loss, and low energy levels, are often linked to folate deficiency. These symptoms can create a vicious cycle, where folate deficiency worsens depressive symptoms, and the symptoms themselves further reduce folate levels. The figure underscores the potential benefits of folate supplementation in improving patient outcomes and advocates for further research to optimize treatment strategies. By addressing folate deficiency, we can uncover a hidden factor in depression and pave the way for more effective, holistic mental health care.
Introduction
In the realm of mental health research, certain trends often dominate the landscape. Over the past few decades, a significant amount of attention has been directed towards understanding the role of serotonin in mood regulation and the genetic factors influencing psychiatric conditions. This focus has led to numerous studies examining the polymorphisms of serotonin-related genes and their potential impact on susceptibility to depression and other mood disorders. While this line of research is undoubtedly important, it has overshadowed another critical area of study: the impact of folate deficiency on mental health (see Figure 1) [1].
Folate, a vital B-vitamin, plays a crucial role in various bodily functions, including DNA synthesis and repair, and the production of neurotransmitters such as serotonin [2]. Despite its importance, the relationship between folate deficiency and depression has not received the same level of attention as genetic research. This blog aims to shed light on the epidemiology, biochemical mechanisms, and clinical implications of folate deficiency in depression, and to advocate for the consideration of folate supplementation as a potential treatment strategy.
The Overlooked Connection Between Folate and Depression
Research dating back to the 1960s has consistently shown a high incidence of folate deficiency among patients with depression. Approximately one-third of individuals with depression exhibit low folate levels, a condition that may be exacerbated by the decreased appetite and weight loss often associated with depressive episodes. While it is clear that folate deficiency is prevalent in this population, the exact nature of the relationship remains a topic of ongoing investigation. Some studies suggest that folate deficiency may contribute to the onset of depression, while others propose that depression itself may lead to reduced folate levels, creating a vicious cycle that hinders recovery (see Figure 1 and 2) [1, 2, 4].
Biochemical Mechanisms Linking Folate Deficiency to Depression
The connection between folate deficiency and depression is believed to involve several biochemical pathways. One key mechanism is the impact of folate on serotonin synthesis. Folate deficiency has been associated with reduced levels of 5-hydroxyindoleacetic acid (5-HIAA), a metabolite of serotonin, in the cerebrospinal fluid of patients with neuropsychiatric disorders. Supplementation with folate has been shown to restore normal 5-HIAA levels, suggesting a direct link between folate status and serotonin production. Additionally, folate is involved in the synthesis of S-adenosylmethionine (SAMe), a compound with known antidepressant properties. SAMe levels are reduced in cases of folate deficiency, further implicating folate in the regulation of mood (see Figure 2).
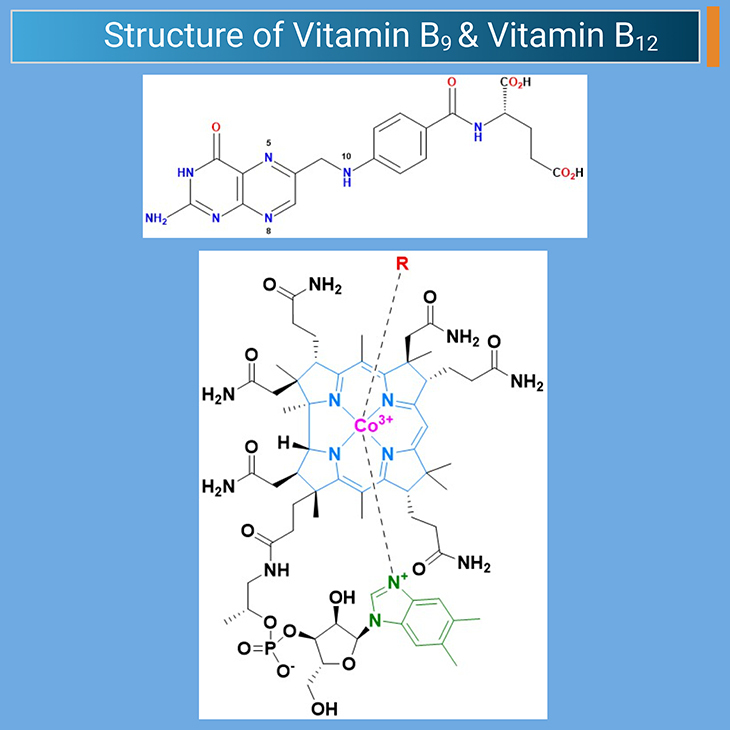
Figure 2: The Nutritional Connection: Unveiling the Impact of Diet on Depression. This figure highlights the intricate relationship between nutrition and depression, emphasizing how dietary factors can influence mental health. Nutrient deficiencies, such as those in folate, vitamin B12, and omega-3 fatty acids, can disrupt neurotransmitter synthesis and function, leading to mood disorders. Folate deficiency (vitamin B9), for instance, is linked to reduced serotonin production, while low levels of vitamin B12 can impair cognitive function and exacerbate depressive symptoms. Omega-3 fatty acids play a crucial role in maintaining neuronal membrane fluidity and modulating inflammatory responses, both of which are vital for mental well-being. The figure underscores the importance of a balanced diet in preventing and managing depression, advocating for further research to optimize nutritional interventions for mental health care. By addressing these nutritional factors, we can enhance overall mental health and improve outcomes for individuals with depression [3 – 4].
The Need for Further Research and Clinical Considerations
Despite the promising evidence linking folate deficiency to depression, more research is needed to fully understand the potential benefits of folate supplementation in this context. Larger studies are required to determine the optimal dosage of folate and to identify which subgroups of patients are most likely to benefit from supplementation. Clinicians must also consider the broader implications of folate supplementation, including the potential need for concurrent vitamin B12 supplementation to prevent masking of B12 deficiency symptoms (see Figure 1 and 2) [1, 2, 3].
Take-Home Messages
High Incidence of Folate Deficiency in Depression
- Research has consistently shown that approximately one-third of individuals with depression exhibit low folate levels, which may be exacerbated by decreased appetite and weight loss associated with depressive episodes.
Biochemical Link to Serotonin
- Folate deficiency is associated with reduced levels of 5-HIAA, a serotonin metabolite, in the cerebrospinal fluid. Supplementation with folate can restore normal 5-HIAA levels, suggesting a direct link between folate status and serotonin production.
Role of SAMe
- Folate is involved in the synthesis of S-adenosylmethionine (SAMe), a compound with known antidepressant properties. SAMe levels are reduced in cases of folate deficiency, further implicating folate in mood regulation.
Need for Further Research
- Larger studies are needed to determine the optimal dosage of folate and to identify which subgroups of patients are most likely to benefit from supplementation.
Folate Supplementation Benefits
- Folate supplementation can lower homocysteine levels even in individuals with normal folate levels. Some subgroups, such as those with the thermolabile variant of MTHFR, may require higher folate levels.
Economic and Clinical Considerations
- Given the low cost of folate tablets, there is no economic reason to avoid giving folate to all depression patients. However, it may be prudent to add a vitamin B12 supplement to avoid masking vitamin B12 deficiency symptoms.
Recommended Dosage
- The recommendation to give 2 mg of folate during the treatment of depression is reasonable, though 1 mg may suffice in countries with food fortification. Adding a vitamin B12 supplement may also be beneficial.
Summary and Conclusions
In conclusion, while the genetic aspects of depression continue to be a major focus of research, it is crucial not to overlook the significant role that environmental factors, such as folate deficiency, can play in mental health. Given the low cost and potential benefits of folate supplementation, it is a strategy that warrants serious consideration in the treatment of depression. By addressing folate deficiency, we may be able to improve outcomes for many patients and provide a more holistic approach to mental health care.
Did You Know? Folate Receptor Autoantibodies (FRAAs) may impede proper folate transport.
Folate (vitamin B9) is very important for your child’s brain development!
During pregnancy, it helps prevent neural tube defects and plays a big role in forming a normal and healthy baby’s brain and spinal cord. Folate also helps cells divide and assists in both DNA and RNA synthesis.
Emerging research suggests that the presence of FRAAs negatively impacts folate transport into the brain.
- Recent studies reveal that a large subgroup of children with autism spectrum disorder (ASD) have FRAAs.
- This suggests that a possible disruption in folate transport across the blood-cerebrospinal fluid (CSF) barrier may potentially influence ASD-linked brain development.
- Screening for the FRAAs in your child should be part of your early intervention strategies.
Is there a test for identifying Folate Receptor Autoantibodies (FRAAs)?
Yes, there is a test – The Folate Receptor Antibody Test (FRAT®) has emerged as a diagnostic tool for detecting the presence of FRAAs.
It is important to screen at an early age or as soon as possible as there may be corrective measures available. Please consult your physician for further information.
To request a test kit, click on the button below.

For information on autism monitoring, screening and testing please read our blog.
References
- Young SN. Folate and depression–a neglected problem. J Psychiatry Neurosci. 2007 Mar;32(2):80-2. PMID: 17353937; PMCID: PMC1810582.
https://pubmed.ncbi.nlm.nih.gov/17353937/
- Bjelland I, Ueland PM, Vollset SE. Folate and depression. Psychother Psychosom. 2003 Mar-Apr;72(2):59-60. doi: 10.1159/000068693. PMID: 12601222.
https://pubmed.ncbi.nlm.nih.gov/12601222/
- Black MM. Effects of vitamin B12 and folate deficiency on brain development in children. Food Nutr Bull. 2008 Jun;29(2 Suppl):S126-31. doi: 10.1177/15648265080292S117. PMID: 18709887; PMCID: PMC3137939.
https://pubmed.ncbi.nlm.nih.gov/18709887/ - Liwinski T, Lang UE. Folate and Its Significance in Depressive Disorders and Suicidality: A Comprehensive Narrative Review. Nutrients. 2023 Sep 4;15(17):3859. doi: 10.3390/nu15173859. PMID: 37686891; PMCID: PMC10490031.
https://pubmed.ncbi.nlm.nih.gov/37686891/


